

Sleep Studies
Sleep studies consist of respiratory polygraphy and polysomnography.
What are respiratory polygraphy and polysomnography?
Respiratory polygraphy means the recording of breathing patterns during sleep. The purpose of this test is to quantify any sleep breathing abnormalities.
Polysomnography additionally analyses the stages (or depth) of sleep as well as its quality by recording the brain’s activity during sleep.
What will having the test entail for my child?
After your child has put on his pyjamas, the following sensors are attached :
- Elastic belts around the chest and stomach: these belts record his breathing by measuring movements of the chest wall and stomach
- A microphone is fixed to the base of the neck with adhesive tape, to record snoring and the airflow passing through the throat
- Another sensor attached to his pyjamas collects information about your child’s position during sleep: on his back, stomach or side, because the quality of sleep can be affected by body position during sleep (breathing is often more difficult when lying on the back)
- The last sensor positioned on the arm gives information on your child’s movements during sleep, to see whether he is awake or moving in his sleep, or whether he is sleeping peacefully
As your child falls asleep:
- A flow sensor resembling tiny glasses will be placed under his nose to record the air flowing in and out
- The concentration of oxygen and carbon dioxide in the blood are recorded by a sensor placed on the tip of the finger for the oxygen sensor and a sensor fixed to the ear or under the nose for the concentration of carbon dioxide. Measuring these two parameters gives information about the impact of nocturnal breathing on gas exchange (such as a drop in oxygen or a rise in carbon dioxide).
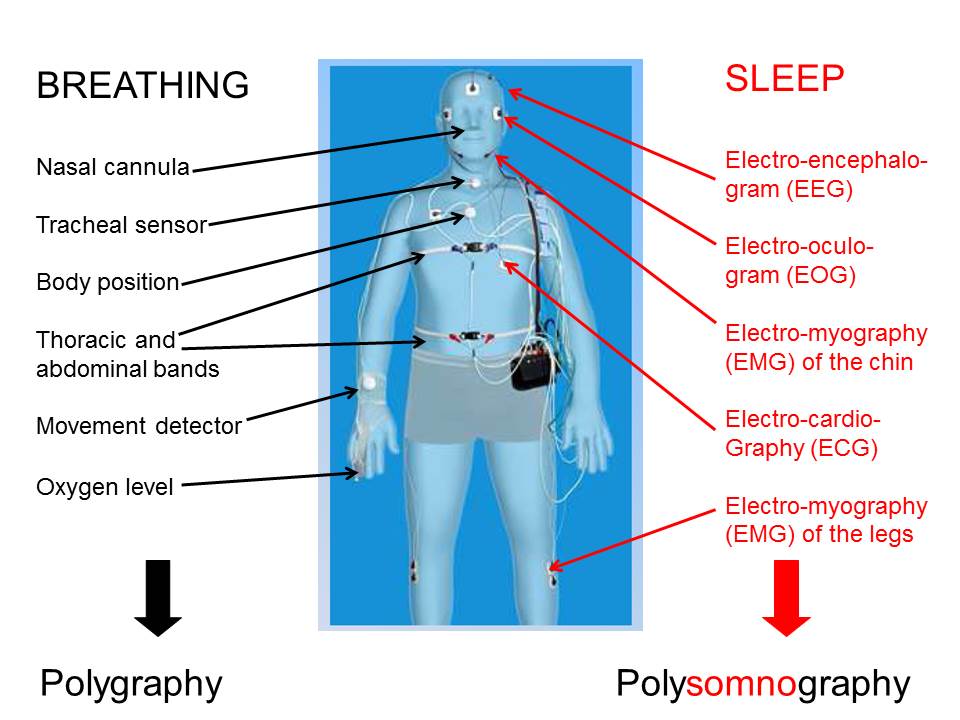
During polysomnography, the following signals are also recorded:
- Recording of the brain’s activity by positioning little cups on the scalp using a sticky paste (washes off in hot water: plan for a hair-wash the following morning), called an electroencephalogram (EEG)
- Recording of the activity of certain muscles by placing sticky tabs on the chin and legs, called an electromyogram (EMG)
- Recording of the activity of the heart by placing sticky tabs on the chest, called an electrocardiogram (ECG)
- Recording of ocular activity by placing sticky tabs close to the eyes, called an electro-oculogram (EOG)
In most cases, an (infra-red) video-camera records your child’s sleep all night long. This recording assists with the interpretation of certain signals over the course of the night. This video recording is exclusively for medical use and only the parts necessary for the interpretation of your child’s tests will be kept.
In young infants (younger than approx. 6 months), sleep studies may alternatively be performed during a day-time nap, if the child is able to sleep for long enough.
What are respiratory polygraphy and polysomnography used for?
Respiraory polygraphy and polysomnography are indicated for the analysis of sleep-induced breathing abnormalities and their impact on the quality of sleep.
The main abnormalities that can occur during sleep are :
- Apnoeas: these are a complete pause of breathing which lasts longer than two normal breaths. These apnoeas may be:
- Obstructive meaning they are linked to a complete closure of the airways
- Central meaning they are linked to a problem with the brain’s respiratory drive
- Hypopnoeas: these are partial closures of the airways
- Desaturations: these are sudden drops in the blood oxygen saturation
Polysomnography will also provide precise information on the exact duration of sleep, its quality, its depth and structure (by providing information on the different stages of sleep), and both conscious and unconscious awakenings. Polysomnography informs us of the impact of breathing abnormalities on the quality of sleep but also of sleep anomalies that have nothing to do with breathing, such as excessive sleep (narcolepsy), insufficient sleep (insomnia), or parasomnia (nightmares, night terrors, somnambulism, bruxism or grinding of the teeth).
There are established norms for all of these events which are different in children and adults. Interpretation of the test therefore has to take into account the child’s age, their medical history and any current medical problems whilst also taking into account the quality of the recording.
What are the main breathing anomalies that occur during sleep?
The principal breathing anomalies are obstructive sleep apnoea syndrome (OSAS) and central sleep apnoea syndrome (CSAS).

Obstructive sleep apnoea syndrome (OSAS)
Recurrent childhood OSAS is a relatively common condition, affecting approximately 1-2% of children between the ages of 3 and 6 years. Enlargement of the tonsils and/or adenoids is the most common cause.
OSAS is associated with nocturnal and day-time signs of variable presence and severity. The nocturnal signs may include:
- snoring
- breathing pauses (apnoeas)
- sweating
- breathing through the mouth
- enuresis (the child wets the bed)
- disturbed sleep
- nightmares
- sometimes abnormal positioning of the head during sleep with the head hyperextended.
Day-time signs may consist of:
- difficulty in waking up
- irritability, hyperactivity, or on the contrary daytime tiredness or drowsiness
- difficulties with attention and memory
- headaches or vomiting
- lack of appetite at breakfast
- growth retardation (which is only found in the most severe cases).
Poor results at school and behavioural problems are the most common and most serious consequences of OSAS, underlining the importance of early, tailored treatment. The cardiovascular (arterial hypertension) and metabolic (metabolic syndrome) impacts of OSAS are mostly encountered in adults, and are less frequent and less severe in children.
Removal of the adenoids and tonsils (tonsillo-adenectomy) is the first-line treatment for recurrent childhood OSAS, resulting in cure in the vast majority of cases. Sometimes a moderate OSAS may persist, especially in a child with obesity or suffering from allergies.
However, OSAS can also occur in a number of rare, genetic conditions or abnormalities. In these situations the signs are often less obvious, the OSAS may be observed at any age and it is often more severe. In a number of conditions, routine sleep testing is recommended. The following list is not exhaustive:
- Conditions associated with a malformation of the face, the maxilla or the mandible (Pierre-Robin syndrome, Goldenhar’s syndrome, Treacher-Collins’ syndrome, cranio-facial stenosis (Apert, Crouzon or Pfeiffer syndromes), pycnodysostosis, but also achondroplasia (or dwarfism), the mucopolysaccharidoses (metabolic diseases) and trisomy 21.
- Conditions associated with anomalies of the tongue, larynx or trachea: stenosis (narrowing) of the larynx or trachea, vocal cord paralysis, floppiness of the larynx (laryngomalacia) or of the trachea (tracheomalacia), Beckwith-Wiedemann syndrome
- Conditions associated with excessive weight or obesity such as Prader-Willi syndrome or ROHHAD Syndrome.
In all of these rare or genetic conditions, management is led by a multi-disciplinary team comprising (depending on the need) ENT surgeons, plastic or maxillo-facial surgeons, oral medicine specialists and orthodontists, neurosurgeons, endocrinologists, geneticists, pulmonary specialists and sleep and respiratory specialists with a special interest in non-invasive ventilation.
Central sleep apnoea syndrome (CSAS)
This syndrome is much less common than OSAS and is found only in certain specific conditions. Central apnoeas can be classified into two groups: genetic conditions and acquired pathologies.
- Genetic causes consist first and foremost of Ondine Curse (central alveolar hypoventilation) which is linked to a genetic defect of the brain’s respiratory drive, but central apnoeas may also be seen in Prader Willi Syndrome.
- The main acquired causes are injury or lesions of the brain or of the spinal cord at the level of the neck such as bony anomalies of the cervico-occipital joints (which may be seen in achondroplasia or the mucopolysaccharidoses), brain tumours, and complications of viral or bacterial infections of the brain.
The symptoms associated with these central apnoeas are much less obvious and often go un-noticed, reinforcing the importance of routine sleep studies in these pathologies.
When and whom should I consult about my child if I suspect sleep-induced breathing disturbances?
Sleep disturbances in general are very common in children. The sorts of sleep disturbances (difficulty in getting to sleep, waking through the night, nightmares) depend on the child’s age. Sleep disturbances of childhood are not all linked to sleep-induced breathing disturbances.
Symptoms that are suggestive of respiratory disturbance are summarised on Pic 7 however they are not specific enough to allow a diagnosis of sleep-induced breathing disturbances with any certainty. If your child manifests several symptoms from Pic 7, even when he doesn’t have a cold, you should discuss this with your paediatrician or GP. The clinician will then perform a thorough physical examination of your child (weight, height) and will check for the presence of enlarged tonsils.
If your child presents a clinical picture suggestive of obstructive sleep apnoea syndrome (presence of suggestive symptoms coupled with enlarged tonsils), he will refer your child to an ENT surgeon.
If your child has symptoms suggestive of obstructive sleep apnoea syndrome but without enlarged tonsils, an ENT opinion is still recommended in order to investigate any potential enlargement of the adenoids (small lymphoid organs located in the nose which can only be visualised with a small camera or with an x-ray).
If your child has a genetic condition and/or a malformation of the airways and/or he has already had the tonsils and adenoids removed, the recommendation is for an opinion in a specialised paediatric centre.
What is the treatment for breathing abnormalities during sleep?
Treatment of obstructive sleep apnoea syndrome (OSAS)
The first-line treatment for common OSAS consists of removal of the tonsils and/or adenoids. This treatment cures the OSAS in the vast majority of cases.
In the event of an associated genetic condition, the treatment will be determined through management by a multidisciplinary team consisting of, depending on the need, an ENT surgeon, a maxillo-facial surgeon, a neurosurgeon, an orthodontist, a paediatric pulmonary specialist, and a specialist in sleep and non-invasive ventilation. Indeed, removal of the tonsils and/or adenoids is rarely sufficient for a complete cure of the OSAS. Depending on the situation, surgical, orthodontic, or non-invasive ventilation treatments may be indicated.
Treatment of central sleep apnoea syndrome
The management of central sleep apnoea syndrome requires a very specific expertise and necessitates specialist management. Depending on the situation, the specialist may call upon medicines, surgery, non-invasive ventilation or a tracheostomy (breathing through a small cannula positioned permanently straight into the trachea).
How does this happen in practice at Necker?
Respiratory polygraphy and polysomnography take place at night in a specially equipped room in the non-ivnasive ventilation and sleep unit. In individual bedrooms, one of the parents is asked to sleep over with the child, so that the study can be performed optimally, with the complete peace of mind of the child.These are individual bedrooms, equipped with a bathroom and a bed for the parent. The investigation can also be performed using portable equipment in a bedroom in a different department within the hospital. The accomodation provided for the parent would then depend on what’s possible within the department concerned.
We ask for you to be present in your child’s bedroom, after having done your child’s admission, at 3pm at the latest so that the sleep unit’s doctor can examine your child and so that the technician has plenty of time to explain the test to your child and to apply all the sensors without rushing.
During the night, a nurse will visit your child regularly to check that everything is going well and that there are no problems with the sensors. Likewise, if you notice a fault with one of the sensors (the sensor has become unstuck or has fallen off), don’t hesitate to inform the nurse.
The following morning, you will be able to leave after the doctor has visited in the late morning. It will not be possible to give you the full results because analysing the test can take a long time. The full results of the test will be posted in 8-15 days at the latest and will be communicated systematically to all of your child’s doctors.